
Gastroparesis: Too Full – Too Long
STEVEN SANDBERG-LEWIS
N.D., DHANP
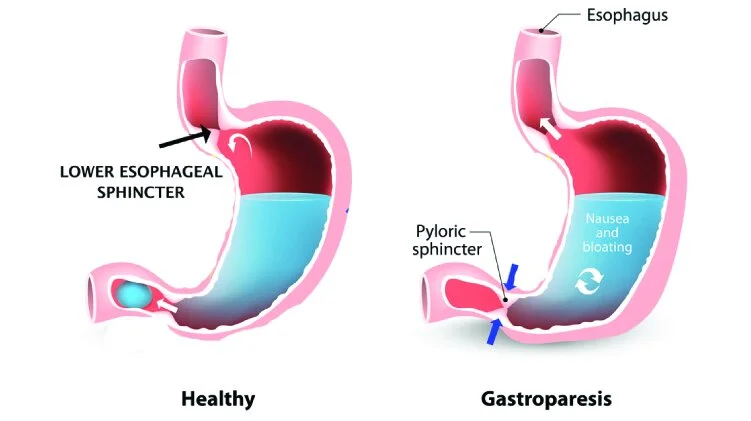
Gastroparesis is a partial paralysis of the stomach which leads to food sitting in the stomach for extended periods of time (delayed gastric emptying). This delayed emptying is quite common in poorly controlled diabetes. Gastroparesis delays the exit of all foods – including carbohydrates- from the stomach and can make it impossible to attain good blood sugar control. It occurs in over half of type I diabetics and in up to one fifth of type II diabetics.
Other gastroparesis triggers or causes include medications, tobacco use, hypothyroidism, several autoimmune diseases, Parkinson’s disease, strokes and traumatic brain injuries. It can also come on after a viral illness or -if no cause is found- gastroparesis may be called “idiopathic”.
Drugs that may cause gastroparesis:
Tobacco
Tricyclic antidepressants
Calcium channel blockers (blood pressure medicine)
L-dopa (Parkinson’s medication)
Hyoscyamine and dicyclomine (antispasmotic medicines)
Narcotics
The symptoms of gastroparesis include nausea or vomiting, bloating, easy fullness when eating, and belly pain. A 4 hour gastric emptying study is the most common method of diagnosis. A test performed in GI motility centers is called antroduodenal manometry and where available it is likely the most accurate diagnostic method. Sometimes evidence of gastroparesis is seen on upper endoscopies, smartpill tests, upper GI barium or small bowel follow-through x-rays.
Diabetics should consider the possibility that they may have gastroparesis if they tend toward low blood sugar one to three hours after meals, high blood sugar five or more hours after meals with no other explanation or inability to control high morning blood sugar levels..
Treatment of gastroparesis:
Diet is key, but it is not only what a person eats, but also how they eat:
Eat in pleasant surroundings
Enjoy the sight and scent of food
Avoid ice cold drinks and foods
Chew food until liquid before swallowing
Eat slowly – unhurried
Avoid eating while driving
Avoid watching television while eating
Practice mindfulness during meals
Some dietary factors that may be key:
Adequate hydration
Smaller more frequent meals
Reduced intake of dietary fiber
Reduced portions of fat per meal
Avoidance of red meat
Reduced protein content at evening meals
Smaller evening meals
Reduced alcohol consumption
Avoidance or limitation of broccoli and other cruciferous vegetables
Gluten-free or grain-free diet
Taking plant medicines such as ginger, artichoke, papaya enzyme tablets or iberogast (a German liquid herb combination) can be very helpful.
Other treatments that are sometimes important include supplementing betaine hydrochloride and/or pancreatic enzymes, certain specific abdominal exercises or chewing gum for the first hour after meals (to increase the production of saliva, stimulate smooth muscle contraction and relax the sphincter at the bottom of the stomach).
Medicines called prokinetics may be prescribed and taken at bedtime or 20-40 minutes before eating. Side effects have caused some of these to be banned by the FDA. I prescribe other, safer prokinetics regularly in my practice. These include tiny doses of erythromycin or prucalopride.
From Kayle Sandberg-Lewis, LMT, MA, BCN-Fellow: Because gastroparesis is often the consequence of one or more traumatic brain injuries, treatment may best be accomplished by addressing the brain injury through neurofeedback. If your gastroparesis came on several days to a few months after a bump to the head or a “slight” whiplash, and you are not responding to the above treatments, seek help from a qualified neurofeedback provider, especially someone using Low Energy Neurofeedback System or LENS – a form of neurofeedback uniquely geared to helping brains recover from injuries.
Steven Sandberg-Lewis, ND, DHANP, has been in clinical practice for 44 years, with a focus on functional gastroenterology. He has been a professor since 1985, teaching a variety of courses but primarily focusing on gastroenterology and GI physical medicine. In 2019, Dr. Sandberg-Lewis co-founded Hive Mind Medicine, continuing his specialization in gastroenterology with a focus on reflux, SIBO, inflammatory bowel disease and functional GI disorders. He is currently working on his latest book, Let's Be Real About Reflux: Getting to the Heart of Heartburn, written to help non-medical and medical professionals alike develop a better understanding of diseases affecting the gastrointestinal tract.
Hive Mind Medicine blog posts are for educational purposes only and are not intended as medical advice. Please consult with your health care practitioner for personalized guidance. Click on the “Learn More” button below if you would like to schedule with one of our Hive Mind practitioners.